Elimination of Tuberculosis: A Feasibility Assessment in Pakistan
This report on the prospects for elimination of Tuberculosis in Pakistan has been created for the WHO Regional Office for the Eastern Mediterranean. An introduction to the global burden of tuberculosis will be followed by a Pakistan specific analysis and targeted control and elimination recommendations.
Introduction to the global burden of tuberculosis
Description
Tuberculosis is an ancient disease, with spinal deformities that are typically associated with tuberculosis having been found in human remains from Egypt and Peru dating back to 5000 BCE.(1) However, tuberculosis (TB) only become epidemic among humans during the seventeenth century when Western Europe saw mass urbanisation, which allowed for a more efficient spread of this airborne disease.(2)
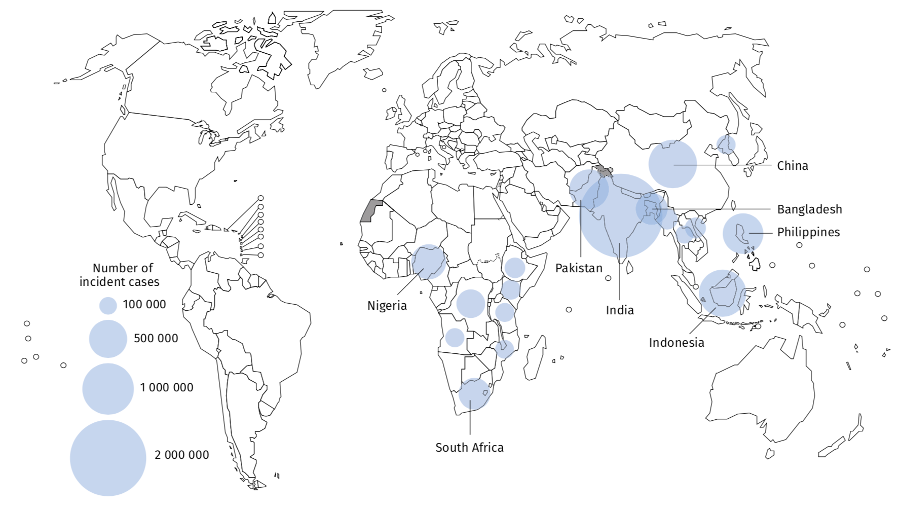
It wasn’t until 1882 that Mycobacterium tuberculosis was discovered as the cause of tuberculosis by Dr. Robert Koch.(3) Since then, almost one quarter of the world is estimated to have been infected by TB, with almost half of this number located in only 8 countries: Bangladesh, China, India, Indonesia, Nigeria, Pakistan, Philippines, and South Africa.(4) Tuberculosis has now overtaken HIV to become the leading cause of death from infectious diseases worldwide,(5) not accounting for the recent COVID-19 pandemic.(6)
Mismanagement of TB treatments have also led to the emergence of multi-drug resistant tuberculosis (MDR-TB). MDR-TB is characterised as TB that has developed resistance to at least two of the front-line antimicrobial TB drugs, isoniazid and rifampicin.(7) Moreover, extensively drug resistant TB (XDR-TB) is characterised as a rare type of MDR-TB with resistance to isoniazid, rifampicin, any fluoroquinolone and at least one second-line injectable drug.(8)
Epidemiology
TB is not region agnostic. In 2020, the WHO South-East Asian region accounted for 43% of new TB cases globally, follow by the WHO African region accounting for 25% of new global cases, then the WHO Western Pacific region with 18% of new global cases.(6)
Over 10 million people contracted TB in 2020, with 1.1 million of those being children.(6) 10 million is also the average number of new cases of TB that occur each year.(6) Within this number, MDR-TB accounts for roughly 440,000 new cases annually, and causes on average 150,000 deaths annually.(2) Catastrophically, there were over 1.5 million deaths due to TB in 2020.(6)
Mycobacterium tuberculosis is spread between people when one infected person coughs, sneezes, spits, sings, speaks, or somehow shares their germs with another person.(4) It is possible to contract TB from inhaling just a few germs.(4) You are more likely to contract it from someone who you live or work with as you are more likely to share greater proximity.(2) Additionally, transmission is a greater risk in overcrowded areas such as slums and prisons.(9)
As previously mentioned, roughly one quarter of the world’s population is infected with Mycobacterium tuberculosis, however, this only means that 2 billion people have the bacteria – not that 2 billion people have active TB.(6) Of those infected with Mycobacterium tuberculosis, their risk of falling ill with active TB is 5-10% across their lifetime.(6) Once ill with active TB, persons are able to infect up to 15 other people with TB bacteria each year.(6)
TB is classified as a poverty-related disease as it disproportionately affects the most vulnerable and marginalised groups wherever the disease is present.(5) Globally, developing countries account for over 95% of all TB cases and deaths.(6) TB is most common in adults in the reproductive stage of their lives,(6) and is more prevalent in males than females.(10) However, there are certain risk factors that increase the risk of developing active TB. A person with a weakened immune system is significantly more likely to develop active TB, and HIV infection increases the risk of developing active TB by 18 times.(6) Undernutrition is another significant risk factor, increasing the risk by a factor of 3 and is responsible for approximately 1.9 million new TB cases globally each year.(6) Misuse of alcohol and tobacco smoking are lifestyle choices that also impact the risk of developing active TB, with the risk increasing 3.3 times and 1.6 times respectively.(6) Together they are responsible for approximately 1.5 millions new cases of TB annually across the world.(6)
Figure 1. Estimated TB incidence in 2020, for countries with at least 100 000 incident cases(11)
Symptoms and Diagnosis
TB most frequently affects the lungs,(12) known as pulmonary TB.(14) However, TB can affect other organs such as the abdomen, skin, joints, lymph nodes, bones, and meninges, in which case a patient is classified as having extrapulmonary TB.(14)
The most common symptoms of TB include: chest pain, a prolonged cough, weight loss and fatigue, fever, and night sweats.(12) However, symptoms of TB may not appear as soon as one becomes infected and can remain mild for many months,(12) causing delays in treatment seeking and possible unconscious spread of the disease.(6) Spread of Mycobacterium tuberculosis is only possible from an active TB patient.(12) If left untreated, TB can cause permanent lung damage, and/or infection of the bones, spinal cord and brain, or even death.(13)
For the initial diagnostic, the WHO recommends rapid molecular diagnostic tests for all people presenting with any symptoms of TB.(6) These tests have high diagnostic accuracy for diagnosing active TB. Diagnosing and detecting MDR-TB or XDR-TB requires bacteriological confirmation of Mycobacterium tuberculosis, as well as culture methods, sequencing technologies or rapid molecular tests to confirm drug resistance.(6) It has also been noted that diagnosing TB in children is more difficult due to the scarcity of bacilli in their specimens, creating insufficient specimen material for testing.(14)
Treatment
Treatment of active TB is typically a 6-month course of a combination of antibiotics.(15) In the first two months, patients take isoniazid, rifampicin, pyrazinamide, and ethambutol. In the last four months, patients only need to take isoniazid and rifampicin.(15) Most people start to feel better and are no longer infectious after 2 weeks of taking the prescribed antibiotics correctly. Skipping a prescribed dose or lack of adherence to treatment plans may cause antibiotic resistant TB infection, known as MDR-TB.
MDR-TB is significantly more difficult to treat and requires a longer course of treatment, up to 9-24 months depending on the level of drug resistance.(11)
Global state of control
TB is both preventable and curable.(6) After two decades of neglection, global prevalence started to decline in the early 1990’s due to the introduction of the Directly Observed Treatment, Short-Course (DOTS) control strategy introduced by the WHO.(5) All countries were recommended to adopt and adapt the DOTS strategy. DOTS was centred on 5 components that are key to TB control: political commitment backed by financing; case detection; standardised, supervised and supportive patient treatment; effective management and supply of drugs; and a standard system for monitoring and evaluating patients and progress.(5) At least 180 countries adopted DOTs and lead to the start of treatment for up to 17 million people by 2003.(5)
Although effective in almost every region of the world, DOTS would not impact the problems of delayed treatment seeking, transmission occurring from undiagnosed patients, or address the increasing pool of people with latent TB.(16) This recognition led to the first Global Plan to Stop TB, covering 2001-2005, in line with MDG goal 6.(5) However, in order to reach the targets set in the MDGs, an enhanced global strategy known as Stop TB strategy was introduced in 2006, which expanded the essential components of the DOTS strategy to also focus on HSS, MDR-TB, HIV co-infection, community engagement and research promotion.(5)
Post 2006, the Stop TB Strategy underpinned the second Global Plan to Stop TB that covered the period 2006-2015.(5) This second Global Plan had ambitious targets to halve the 1990 TB prevalence and mortality rate by 2015 and eliminate TB by 2050.(17) From 2016-2020 the Stop TB Partnership’s Global Plan to End TB introduced the 90-90-90 targets in line with new SDG targets.(18) The targets were: to reach 90% of people with TB and start them on appropriate treatment, including at least 90% of the most vulnerable and at-risk people, and achieve a treatment success rate of at least 90% by 2020.(18)
In light of progress up to 2015, the 2014 World Health Assembly announced intensified TB elimination targets, with the goal to eliminate the TB epidemic by 2035, including reducing mortality by 95%, reducing incidence by 90%, and minimising the catastrophic costs for patients and their families.(19) The 2016-2035 End TB Strategy has 3 key pillars: integrated patient-centred care and prevention; supportive systems and bold policies; and intensified research and innovation efforts.(5)
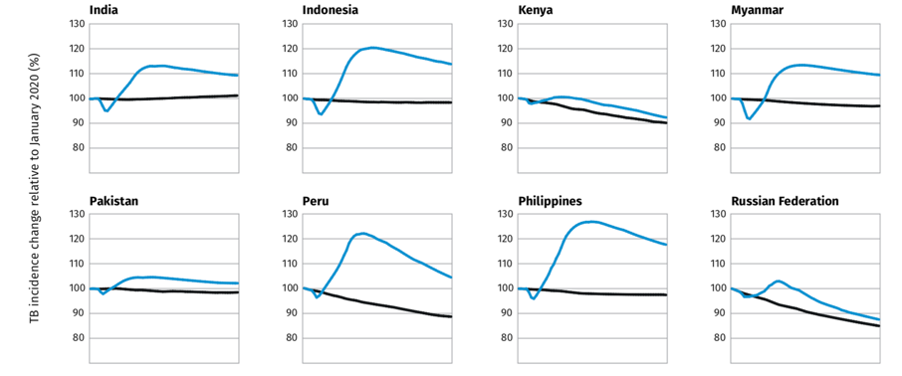
COVID-19 has however caused a dramatic drop in case notifications during 2020, with at least 3 million less people being newly diagnosed with TB and reported compared to pre-2020 estimates.(11) TB incidence rates still averaged around 10 million, which takes us back to an incidence reporting rate equal to that of 2012.(11) TB deaths have also increased by an estimated 0.2-0.4 million.(20)
Figure 2. Estimated impact of the COVID-19 pandemic on TB incidence, up to 2025(11)
Standardized TB incidence rate

Tuberculosis in Pakistan
Tuberculosis is highly endemic to Pakistan.(21) With a population of approximately 197 million people, Pakistan is currently ranked 5th for highest TB incidence worldwide,(22) and accounts for up to 61% of the TB burden in the WHO Eastern Mediterranean Region.(24)
Epidemiology
Pakistan estimates there are approximately 525,000 new TB cases annually, including approximately 27,000 MDR-TB cases.(12) However, in 2018, just under 370,000 people were diagnosed with TB, and 15,000 with MDR-TB.(23) This leaves a gap of up to 160,000 people who are likely undiagnosed and very unlikely to be receiving treatment. An estimated 56,000 deaths from TB occur each year in Pakistan.(25)
Of the 369,548 notified cases of TB in Pakistan during 2018:
- 20% had a known HIV status,
- 80% were diagnosed with pulmonary TB,
- 48% of cases were confirmed bacteriologically,
- 13% of cases were in children under 15 years,
- 42% of cases were in women, and
- 45% of cases were in men.(23)
However, another report estimated that childhood prevalence of TB in Pakistan is as high as 20%.(26)
In line with global trends, more males than females are infected with TB in Pakistan, however, there was no significant gender correlation for MDR-TB or extrapulmonary TB.(21) Low socioeconomic status and education level are the primary risk factors associated with TB infection in Pakistan.(12) The treatment success rate for TB currently ranges between 70-94%.(12)
MDR-TB in Pakistan is estimated to account for 4.2% of new TB cases and 16% in patients who have been previously treated for TB.(21) On average, 65% of MDR-TB patients in Pakistan complete their treatments, although this success rate varies widely between regions despite standardised treatments.(12) The Khyber Pakhtunkhwa (KPK) region reported a success rate between 63-79%, Rawalpindi city reported a 10% success rate, and Karachi reported a 39% success rate.(12) The primary risk factors for MDR-TB in Pakistan are reported to be age between 15-25 years, male gender, less than 5 years of formal schooling, and Sindhi ethnicity.(27)
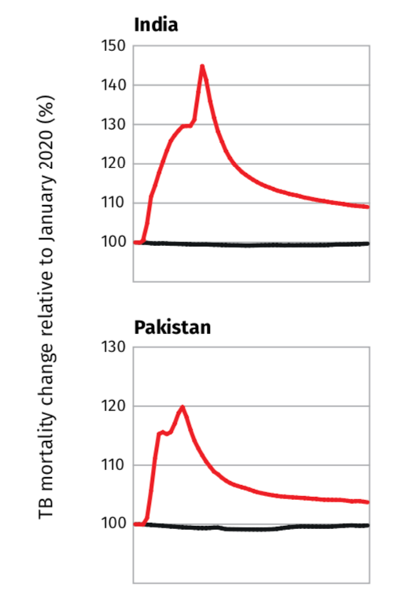
Although the impacts of COVID-19 on TB incidence and mortality numbers in Pakistan are not yet conclusive due to the ongoing nature of the COVID-19 pandemic, the WHO has released it’s expected mortality impact (Figure 4).
Figure 3. Political Map of Pakistan(28)

Figure 4. Estimated impact of the COVID-19 pandemic on TB mortality, up to 2025(11)
Standardised TB mortality rate (including HIV)

Case definitions
Pakistan was one of seven countries that agreed to test the definitions and forms of TB to underpin the official WHO standard case definitions.(29) These definitions were last revised in January 2020. The two primary case definitions used in this report, and in Pakistan, are:
- Bacteriological: “A bacteriologically confirmed TB case is one from whom a biological specimen is positive by smear microscopy, culture or WRD (such as Xpert MTB/RIF).”(29) All bacteriologically confirmed TB cases must be notified, regardless of the treatment status.
- Clinical: “A clinically diagnosed TB case is one who does not fulfil the criteria for bacteriological confirmation but has been diagnosed with active TB by a clinician or other medical practitioner who has decided to give the patient a full course of TB treatment… including cases diagnosed on the basis of X-ray abnormalities or suggestive histology and extrapulmonary cases without laboratory confirmation.”(29) If a clinically diagnosed TB case is later confirmed bacteriologically, it needs to be reclassified as bacteriologically confirmed.
Clinically diagnosed or bacteriologically confirmed cases of TB may also be classified according to:
- The anatomical site of TB – the difference between pulmonary and extrapulmonary TB;
- HIV status – a significant risk factor for TB infection; and
- Treatment history and drug resistance – a significant risk factor for MDR-TB.(29)
Local control strategies
Until the Islamabad declaration of a national TB emergency and the revival of the National TB Control Program (NTP) in 2001, TB control in Pakistan was limited.(23) This revival led to an initial 5-year plan to 2005, with the aim to roll-out universal DOTS coverage for the Pakistan public sector. With support from the Global Fund, the roll-out of universal DOTS coverage across the country was a success and the program scope was extended post 2005 to include coverage for MDR-TB.(23,30) The NTP has a goal to reduce the prevalence of TB in the general population by 50% by 2025 compared to 2012 levels.(31) The Government of Pakistan also had an ambitious goal to achieve zero deaths attributable to TB and universal access to care for TB by 2020.(23) According to current trends and the latest published data, the Government of Pakistan did not meet its goal and the NTP is not on track to meet its 2025 goal.(23,27) To date, the Government has not released revised targets and the NTP is several years behind in its annual reporting.(23)
Although the NTP’s plan focussed primarily on DOTS coverage in the public sector, there are currently over 1700 public and private sector facilities across the country delivering free diagnostic and treatment services for TB.(23) Additionally, there are at least 34 Programmatic Management of Drug Resistance TB treatment sites (PMDT) for MDR-TB across Pakistan.(12) Approximately 85% of Pakistani patients select the private sector as their preferred healthcare provider, however less than one percent of private sector providers report cases of TB to the NTP.(23)
In the current COVID-19 climate, Pakistan has been credited for their successful adaptations to the NTP strategy. The key adaptations were providing TB medications for longer periods of time to reduce the number of visits to health care facilities; increased training on the use of PPE, and online modules on infection control; and the recent engagement of Lady Health Workers (LHW’s) to address stigma and fear in rural communities.(20)
As of 2021, the NTP have announced that mandatory TB Case Notification Acts have been approved in the Provinces of Sindh, KPK, and Punjab, and will commence one-year pilots in five districts with the support of the Global Fund.(32) The NTP is also supporting Provinces to establish their own online TB case notification programs through NTP helpline.(32)
Challenges in local control
This report has identified three key challenges that are impacting the current state of TB control in Pakistan.
Low levels of education
Pakistan currently has the second highest number of out-of-school children (OOSC) in the world, with 22.8 million, or 44%, of 5-16 year-olds not attending school.(33) An approximate 12 million children drop out of school between primary and lower secondary schooling levels.(33) Socio-economic status, gender, and geography are significantly correlated with level of educational attainment; 52% of the poorest children, of which 58% are girls, are OOSC in the Sindh Province, and 78% of girls in the Balochistan Province do not attend school.(33) Limited education in the primary years affects comprehension levels, and can lead to misunderstanding of disease impact and treatment, and drug misuse.(12)
Travel distances and associated costs
Before COVID-19 brought the world to a standstill and delayed many aspects of life, TB patients in Pakistan often delayed or completely avoided treatments due to the time and costs associated with travelling.(34) Studies have found that patients can spend up to 3 hours travelling to treatment centres, and spend an additional 3-4 hours waiting for treatment at those centres.(12) Oftentimes, travelling long distances is a costly venture, and patients report experiencing fatigue and weakness whilst travelling.(34) Additionally, travelling in Pakistan is more challenging for females due to limited freedoms.(12)
Underreporting
Studies suggest that there is significant underreporting and/or under-detection of TB cases in Pakistan, especially among the elderly and men.(16) Additionally, less than one percent of private treatment centres report TB cases to the NTP.(23) This significantly affects TB case detection, reporting, treatment and control of TB within Pakistan.
Recommendations for TB elimination in Pakistan
Prospects for disease control
Whilst the NTP has taken great measures to adapt their TB strategy during COVID-19, it is not apparent whether the adaptations are permanent additions to the NTP. This report recommends the NTP make these adaptations permanent. Additionally:
- The Government of Pakistan should put pressure on the private sector to increase their TB case reporting rates. As men have more access to healthcare, and over 85% of Pakistani patients elect private health providers, this has the potential to significantly decrease the gap between the estimated number of TB infections and the number of TB infections reported. The NTP provides free diagnostics and treatments to any patients that present to treatment centres and is supported by the Global Fund, so the Government is unlikely to incur significant costs. However, if the Government were willing to underpin this approach by investing in active screening of at-risk people in rural areas (such as people infected with HIV or undernourished), a significant impact on community incidence rates could occur alongside improvements in TB treatment adherence and reduced incidences of MDR-TB.
- National TB control efforts would significantly improve on average if treatment adherence efforts were increased in Rawalpindi and Karachi. Providing financial incentives for patients to adhere to their treatments has been proven successful with patients with psychotic disorders.(35) The same theory is likely to have success in Pakistan with financial support from the Government.
Prospects for disease elimination
- LHW’s are trusted health workers in rural communities and are relied upon to supply rural communities with appropriate health information. In addition to the recent engagement of LHW’s to address the stigma of TB, significant progress towards TB elimination could be made if the NTP enabled LWH’s to carry drugs to their patients in rural communities. Time and costs associated with travelling to treatment centres is currently a serious deterrent in seeking health care and treatment. By supporting LHW’s to bring treatments to their patients, more patients are likely to have access to TB treatments, especially females and children, and adherence to treatment schedules is likely to increase due to the convenience of available drugs. This is a more cost-effective solution than recommending the establishment of rural drug centres and can positively impact female employment rates overall if the initiative is appropriately supported and scaled up.
- Perhaps the only benefit from the COVID-19 pandemic is that global awareness of the importance of hand-washing, social distancing, masks and ventilation for airborne diseases has dramatically increased. This report recommends that the Government of Pakistan focus on increasing the number of children who continue their education past the primary level. As the impacts of the COVID-19 pandemic are so profound, it is reasonable to assume that education surrounding airborne disease prevention is at least adequate in all corners of the world. For this reason, focussing on increasing general educational attainment for children, and relying on existing education surrounding disease control, could make strides in improving the social determinants of health overall. Whilst this recommendation is extremely costly and would not see improvements for, likely, generations to come, it would improve the overall development of Pakistan.
Prospects for disease eradication
Eradication of TB in humans at this time is extremely unlikely until significant progress has been made towards the global End TB Strategy. This is because the risk of transmission from patients from other countries cannot be ruled out until elimination of TB in all countries is achieved.
Final Note
After critical review of the literature, this report concludes that the prospects for TB elimination in Pakistan are moderately positive. The primary recommendations of this report are government pressure on the private sector and the enablement of LHW’s to transport drugs to rural patients for their relative cost-effectiveness and ability to take the burden of disease management off patients. Further research would benefit from exploring the viability of financial incentives for treatment adherence success and ability to proactively screen vulnerable people at risk of TB infection.
References
- Gerszten PC, Gerszten E, Allison MJ. Diseases of the spine in South American mummies. Neurosurgery. 2001 Jan 1;48(1):208-13.
- Talbot EA, Raffa BJ. Mycobacterium tuberculosis. Molecular medical microbiology 2015 Jan 1 (pp. 1637-1653). Academic Press.
- Tuberculosis (TB) – World TB Day – History [Internet]. Centers for Disease Control and Prevention. 2021 [cited 10 October 2021]. Available from: https://www.cdc.gov/tb/worldtbday/history.htm
- Tuberculosis [Internet]. Who.int. 2021 [cited 10 October 2021]. Available from: https://www.who.int/health-topics/tuberculosis#tab=tab_1
- Sulis G, Roggi A, Matteelli A, Raviglione MC. Tuberculosis: epidemiology and control. Mediterranean journal of hematology and infectious diseases. 2014;6(1).
- Tuberculosis (TB) [Internet]. Who.int. 2021 [cited 10 October 2021]. Available from: https://www.who.int/news-room/fact-sheets/detail/tuberculosis
- World Health Organization. WHO consolidated guidelines on drug-resistant tuberculosis treatment. World Health Organization; 2019.
- Multidrug-Resistant Tuberculosis (MDR TB) [Internet]. Centers for Disease Control and Prevention. 2021 [cited 10 October 2021]. Available from: https://www.cdc.gov/tb/publications/factsheets/drtb/mdrtb.htm
- Houben RM, Dodd PJ. The global burden of latent tuberculosis infection: a re-estimation using mathematical modelling. PLoS medicine. 2016 Oct 25;13(10):e1002152.
- Neyrolles O, Quintana-Murci L. Sexual inequality in tuberculosis. PLoS medicine. 2009 Dec 22;6(12):e1000199.
- Global Tuberculosis Report 2021 [Internet]. Who.int. 2021 [cited 17 October 2021]. Available from: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2021
- Iqbal F, Defer MK, Latif A, Hadi H. Understanding how geographic, demographic and treatment history impact health outcomes of patients with multi-drug-resistant tuberculosis in Pakistan, 2014–2017. Epidemiology & Infection. 2020;148.
- Tuberculosis (TB) | Cedars-Sinai [Internet]. Cedars-sinai.org. 2021 [cited 20 October 2021]. Available from: https://www.cedars-sinai.org/health-library/diseases-and-conditions/t/tuberculosis-tb.html
- Elhassan MM, Elmekki MA, Osman AL, Hamid ME. Challenges in diagnosing tuberculosis in children: a comparative study from Sudan. International Journal of Infectious Diseases. 2016 Feb 1;43:25-9.
- Tuberculosis (TB) – Treatment [Internet]. nhs.uk. 2021 [cited 23 October 2021]. Available from: https://www.nhs.uk/conditions/tuberculosis-tb/treatment/
- Wejse C. Tuberculosis elimination in the post Millennium Development Goals era. International Journal of Infectious Diseases. 2015 Mar 1;32:152-5.
- World Health Organization. The global plan to stop TB, 2006-2015. World Health Organization; 2006.
- Stop TB Partnership [Internet]. Stoptb.org. 2021 [cited 25 October 2021]. Available from: https://www.stoptb.org/about/
- World Health Organization. The End TB Strategy. Global strategy and targets for tuberculosis prevention, care and control after 2015. World Health Organization. 2014.
- Fatima R, Akhtar N, Yaqoob A, Harries AD, Khan MS. Building better tuberculosis control systems in a post-COVID world: learning from Pakistan during the COVID-19 pandemic. International Journal of Infectious Diseases. 2021 Mar 17.
- Ali S, Khan MT, ANWAR SHEED KHAN NM, KHAN MM, AHMAD S, NOOR S, JABBAR A, CANTILLON DAIRE FH. Prevalence of multi-drug resistant Mycobacterium tuberculosis in Khyber Pakhtunkhwa–a high tuberculosis endemic area of Pakistan. Polish journal of microbiology. 2020 Jun;69(2):133.
- Waheed Y, Khan MA, Fatima R, Yaqoob A, Mirza A, Qadeer E, Shakeel M, Heldal E, Kumar AM. Infection control in hospitals managing drug-resistant tuberculosis in Pakistan: how are we doing?. Public health action. 2017 Mar 21;7(1):26-31.
- TB in Pakistan [Internet]. Tbfacts.org. 2021 [cited 27 October 2021]. Available from: https://tbfacts.org/tb-pakistan/
- Tuberculosis [Internet]. World Health Organization – Regional Office for the Eastern Mediterranean. 2021 [cited 28 October 2021]. Available from: http://www.emro.who.int/pak/programmes/stop-tuberculosis.html
- Hashmi F. TB Online – TB cases on the rise in Pakistan [Internet]. Tbonline.info. 2019 [cited 28 October 2021]. Available from: https://www.tbonline.info/posts/2019/4/21/tb-cases-rise-pakistan/
- Subregional workshop on childhood tuberculosis (TB), 13–17 May 2013 [Internet]. World Health Organization – Regional Office for the Eastern Mediterranean. 2021 [cited 28 October 2021]. Available from: http://www.emro.who.int/pak/pakistan-events/sub-regional-workshop-on-childhood-tb.html
- Ahmad AM, Akhtar S, Hasan R, Khan JA, Hussain SF, Rizvi N. Risk factors for multidrug-resistant tuberculosis in urban Pakistan: A multicenter case–control study. International journal of mycobacteriology. 2012 Sep 1;1(3):137-42.
- Political Map of Pakistan, Pakistan Provinces Map, Pakistan Political Map [Internet]. Mapsofworld.com. 2020 [cited 1 November 2021]. Available from: https://www.mapsofworld.com/pakistan/pakistan-political-map.html
- World Health Organization. Definitions and reporting framework for tuberculosis–2013 revision: updated December 2014 and January 2020. World Health Organization; 2013.
- Global Fund Grants in the Islamic Republic of Pakistan [Internet]. Theglobalfund.org. 2020 [cited 1 November 2021]. Available from: https://www.theglobalfund.org/media/9595/oig_gf-oig-20-012_report_en.pdf
- About Us [Internet]. National TB Control Programme – Pakistan. 2021 [cited 1 November 2021]. Available from: https://ntp.gov.pk/about-us/
- NTP STARTS TB CASE NOTIFICATION PILOT PROJECT IN FIVE DISTRICTS OF PAKISTAN [Internet]. National TB Control Programme – Pakistan. 2021 [cited 1 November 2021]. Available from: https://ntp.gov.pk/2020/01/21/ntp-starts-tb-case-notification-pilot-project-in-five-districts-of-pakistan/
- Education [Internet]. Unicef.org. 2021 [cited 2 November 2021]. Available from: https://www.unicef.org/pakistan/education
- Khan A, Walley J, Newell J, Imdad N. Tuberculosis in Pakistan: socio-cultural constraints and opportunities in treatment. Social science & medicine. 2000 Jan 1;50(2):247-54.
- Priebe S, Yeeles K, Bremner S, Lauber C, Eldridge S, Ashby D, David AS, O’Connell N, Forrest A, Burns T. Effectiveness of financial incentives to improve adherence to maintenance treatment with antipsychotics: cluster randomised controlled trial. Bmj. 2013 Oct 7;347.